
In honor of the 4th of July holiday, I thought I’d squeeze in one more post – let’s talk about IMMUNOTHERAPY, which has created fireworks of its own in the cancer treatment world!
In order to talk about the exciting clinical trials and ideas that are out there for sarcoma patients, we need to first review a little bit about the immune system and how it is supposed to fight cancer.
The immune system is designed to defend the body against all invaders, foreign and domestic. In addition to fighting off nasty cold viruses and ripe bacteria in your sushi, it is also constantly surveying your own cells in order to detect damaged or cancerous cells and destroy them.
Let’s walk through a flu infection and review the several types of white blood cells that are important to know about in understanding the immune response. The flu viruses are made up of protein particles (antigens). When flu viruses enter the body, those protein particles floating around in your nose and mouth and lungs are picked up and processed by immune cells called “antigen-presenting cells”, including macrophages and dendritic cells. Just like your tattling younger siblings, the APCs pop the flu virus particles onto their surface and show them to the immune cells in charge. These “parental” immune cells are called T-cells. They decide that those flu proteins are evidence of a foreign invader, and need to be destroyed. They do this by launching a series of signals to recruit other T-cells and kickstart other immune processes (antibodies) to seek out that specific type of protein and destroy whatever it is attached to. Eventually, with enough “Flu-specific” T-cells floating around, all the flu viruses are detected, killed off, and cleaned up, and the body returns to normal. Even more amazingly, the body retains a few T-cells that remain “educated” about the flu virus, as memory T-cells, so that should that flu particle ever show up again, it is quick and easy to recruit and direct the immune response avoiding another all-out infection. Flu viruses change from year to year, which is why the flu vaccines are always slightly different and you need a new one each year, and also why you can get flu over and over again.
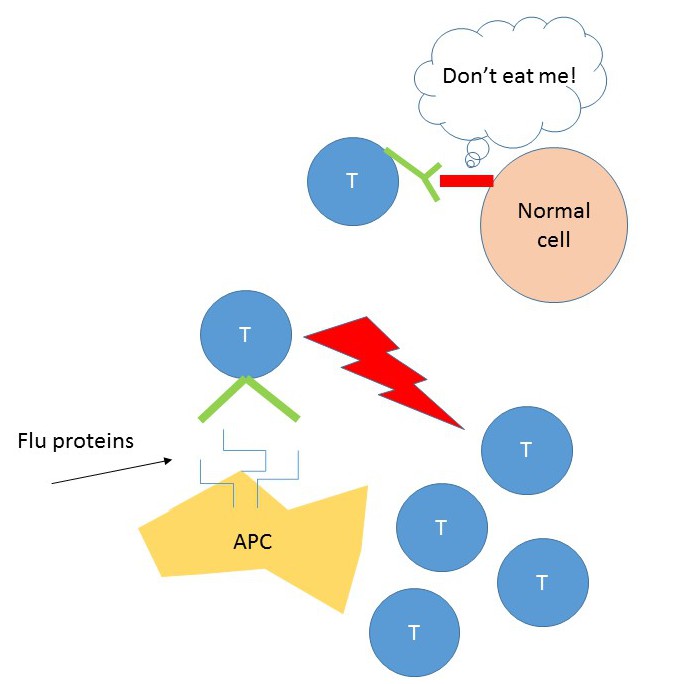
Similarly, a special fraction of T-cells are specifically designed to recognize cancer cells in your body. In an analogous way, if a cancer cell is detected, immune cells arrive at the area and launch signals that either kill the cell, or induce it to kill itself off. Importantly, normal cells have a variety of signals (called immune “Checkpoints”) to divert the T-cells away and ensure that the immune system doesn’t mistakenly start killing off your own healthy cells.
So here’s the situation in cancer. The first cancer cell of a tumor somehow escapes recognition and destruction by a T-cell and it is able to continue to divide and grow until it forms a solid tumor ball of tumor cells. The whole concept of immunotherapy, in a nutshell, is to try various treatments that can reeducate the immune system to recognize and attack the tumor cells. In theory, if you could do this, the natural mechanisms of recruitment of lots of cancer-cell specific T-cells and long-lasting memory T-cells should kick in, and you could potentially cure cancer, like you can recover from an attack of the flu.
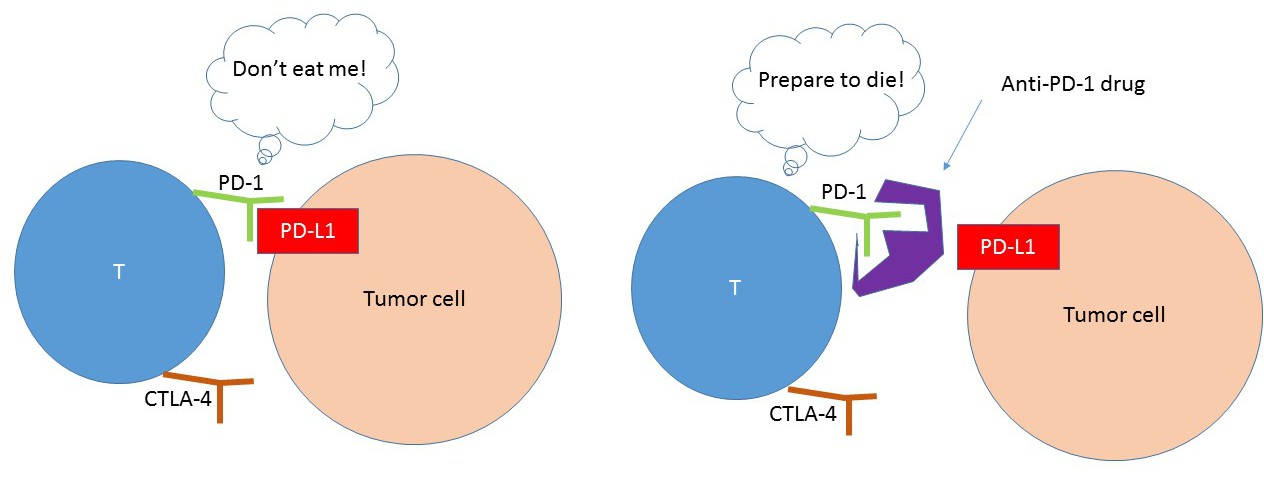
How can we do this? There are a few ways. First, we’ve learned that in some cancers, the tumor cells have evolved the ability to exhibit the SAME “Don’t-eat-me” checkpoint signals that normal cells use to avoid the immune system. The most famous checkpoint proteins are PD-1 (on the T-cell) and PD-L1 (on the tumor cell). The pharmaceutical companies have developed drugs that block the interaction between the tumor cell and the T-cell – the two PD-1 blocking drugs that are approved by the FDA are called pembrolizumab (Keytruda) and nivolumab (Opdivo). There are also several anti-PD-L1 drugs in development. Large clinical trials have shown that SOME PATIENTS (not all) with melanoma, non-small cell lung cancer, kidney cancer, liver cancer (not cancer that has spread to the liver), bladder cancer, and certain types of colon cancer can have dramatic results from anti-PD1 therapy. What is peculiar is that in some patients, it doesn’t work at all. As you might imagine, all of these patients had their tumors tested to see whether they actually had the “don’t-eat-me” flag, or PD-L1. While the chance of a patient benefiting from anti-PD1 therapy was a lot better if they DID have PD-L1 on their tumors, there were some patients that did not respond even though their cancer HAD PD-L1, and some that didn’t have it but still responded. So this is still very confusing and a lot of very smart people are trying to figure out why this is the case.
There are a few possible explanations. First, immune therapy takes time to work. In many patients, the tumors actually increased in size while on treatment, and some patients were even removed from the trial drug. However, they still lived longer and sometimes there was a delay in being able to see tumor shrinkage. If the tumors are growing very quickly, there just may not be enough time for the immune system to wake up and go after the tumor cells before you run into serious trouble. Also, remember that you need T-cells to actually be IN the tumor for PD-1 blocking therapy to make sense. If you block PD-1, but there are no T-cells around the tumor cells to recognize them, or if the T-cells are not functioning well (can happen after heavy chemotherapy), they might not be able to launch an effective, tumor-specific response. Many large tumors, especially sarcoma, might have lousy blood flow into the middle of them, so there might not be enough delivery of immune cells onto the front lines. Thus, many people are thinking that it might not be PD-L1 that is important, but whether you have T-cells in the vicinity of the tumor (particularly T-cells with PD-1 on them) to predict who is likely to respond well.
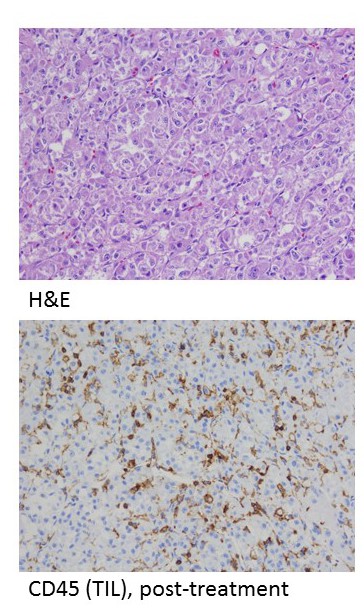
To the left is a picture of a sarcoma with a lot of immune cells nestled in and around the tumor cells- the top picture shows sheets and sheets of tumor cells, the bottom picture shows brown staining T-cells (TIL – stands for tumor-infiltrating lymphocytes)
There are also dozens and dozens of other surface checkpoint proteins that might be important that have barely been studied. Finally, not all tumor cells are the same. When they stain the tumor slices for PD-L1, it’s common to see it in some areas and not in others. Plus, just like next seasons’ flu viruses, tumor cells vary in their particular proteins even within the tumor. Complicated… So now there are even more excited people trying to combine PD-L1 blockers with other treatments to make it work better. For example, in kidney cancer, studies have found that combining PD-1 therapy with a small anti-blood vessel drug like sunitinib seemed to help the immune system work better. However, the side effects from doing this were significant.
The other thing to know is that the side effects of anti-PD-1 treatments can be significant. By taking down the checkpoint that keeps the immune system at bay, your normal cells are subject to attack as well as the cancer cells. Inflammation of a variety of normal cells can occur, including the lungs, colon, thyroid, liver, and a host of other organs. These side effects can be severe and require steroids to suppress the immune system again.
So what about sarcoma? Way back in the 1890s, Dr. Coley (photo on right) reported that a patient who had sarcoma was cured after he had a severe bacterial infection. Presumably the sarcoma cells got caught in the crossfire from the huge immune response to the bacteria. He actually injected patients with Streptococcus bacteria later on, trying to cure sarcomas. Convenient… but certainly doesn’t happen every time.
Another thing that is interesting is that a few patients with sarcoma can be cured, even if they had widespread disease and clearly had tumor cells floating around- making us wonder if the number of sarcoma cells gets low enough, the immune system can smarten up and take over. Thus, scientists who have been working on immunotherapy have been interested in sarcomas for a while. For the checkpoint inhibitors like anti-PD-1, clinical trials are just starting for sarcoma patients – in fact the first one filled up in only three months. Crazy. And now we wait for the results… however there are a few other ones out there now, and more on the horizon.
Other ways that scientists have tried to unleash the immune system include vaccines. Kind of like a flu shot, people have tried to inject particles that stimulate the immune system in hopes of going after the cancer cells. And in some cases, scientists have actually harvested T-cells, engineered them with proteins or tumor bits, and returned them to the patients. For example, Dr. Rosenberg’s group at the NIH has given T-cells specifically “educated” to go after a protein called NY-ESO to patients with synovial sarcoma – these tumors often express the NY-ESO protein. There have been some exciting responses – but again, not everyone. My colleague Dr. John Goldberg has an ongoing clinical trial here at the University of Miami, where we harvest immune cells from a patient with sarcoma, engineer them to become super dendritic cells, load them with pieces of the patient’s own tumor that has been surgically removed, and give them back to the patient. We even give “booster” shots of tumor proteins every month or so after completion of the vaccine protocol. Exciting stuff!
What would be really cool is if we could somehow combine all of these techniques – combine PD-L1 blockade with vaccine therapy to unleash a mega-immune response specific to the tumor – and as we learn more about which patients may respond from the ongoing trials, we can customize.
So I hope that I have gotten you at least a little excited about the potential of immunotherapy. The take-home point is that we still have a LONG way to go to understand the best way to train the immune system to go after cancers. Although the media has painted immunotherapy as the way to cure cancer, it’s important that we understand what the story really is at this point. Only a few of the patients have gone on to long remissions – and the insurance companies have not been willing to support the high costs for any cancers without drug approval. The critical piece is to open more clinical trials and get patients on them- that way we can be sure to learn as much as possible about who is really benefiting and avoid false hopes and unnecessary side effects.
Happy weekend!
Referenced immunotherapy trials for sarcoma patients:
Pembrolizumab for bone and soft tissue sarcomas (mostly full as I understand)
Nivolumab for advanced uterine leiomyosarcomas
Nivolumab with or without ipilimumab in younger patients with recurrent or refractory sarcomas (part 1, 18 years or younger, part 2 up to 30 years- Ewings, rhabdo, osteo)
photo credit: William Coley – https://en.wikipedia.org/wiki/William_Coley

It’s not just anyone who can get me to “walk through a flu infection” with her – argh! – but I’ve said it before, and I’ll say it again – I’ll follow you anywhere, Dr. Bree! Thank you for all the helpful illustrations and explanations! Such exciting stuff!
LikeLike
Wow! Great explanation that even a totally non-scientist like me can understand. Exciting! My AS basically “disappeared” (NED) after AIM and taxol. Unusual I am told.
LikeLike
Pingback: Updates from ASCO 2017 Annual Meeting – breelynwilkymd
Pingback: Leiomyosarcoma in 2018 – where we are and where we need to go. – breelynwilkymd
Pingback: Updates from ASCO – 2019 | breelynwilkymd
Pingback: Shining the Spotlight on Synovial Sarcoma… | breelynwilkymd