 Greetings, and humble apologies for the hiatus of this blog – have not forgotten about all of you, but it’s been a crazy year in the world of sarcomas. I’m so excited to share with you some of the highlights of ASCO, where nearly 40,000 medical oncologists and other cancer research aficionados gather yearly to present the most updated cancer research. Without further ado, here are summaries of the most interesting and important abstracts and presentations from the sarcoma sessions.
Greetings, and humble apologies for the hiatus of this blog – have not forgotten about all of you, but it’s been a crazy year in the world of sarcomas. I’m so excited to share with you some of the highlights of ASCO, where nearly 40,000 medical oncologists and other cancer research aficionados gather yearly to present the most updated cancer research. Without further ado, here are summaries of the most interesting and important abstracts and presentations from the sarcoma sessions.
Dr. Sant Chawla from the Sarcoma Oncology Group in Santa Monica presented the results of a Phase III trial comparing aldoxorubicin vs. investigator’s choice of chemotherapy, which could include pazopanib, gemcitabine/docetaxel, dacarbazine, doxorubicin, or ifosfamide. What’s aldoxorubicin? It is doxorubicin, the backbone of most sarcoma chemotherapy combinations, but it binds to the blood protein albumin as soon as it gets in the body. This allows it to travel in an inactive form to the tumor site without damaging normal cells as much as regular doxorubicin along the way, until it enters the low-oxygen and acidic state within the tumor, where it breaks off the albumin and can go to work. In particular, aldoxorubicin doesn’t seem to damage the heart nearly as much as regular doxorubicin can, which allows much more of the drug to be given compared to doxorubicin. In this study, the rates of a drop in cardiac “squeeze” were only 4.2% vs. 19.1% in the patients that received regular doxorubicin in the investigator’s choice arm. 
But does it work? 433 patients were included on this study with leiomyosarcoma, liposarcoma, synovial sarcoma as well as a smattering of “other” subtypes who had never received any chemotherapy before for metastatic disease. In general, there was modest improvement in the aldoxorubicin treatment group compared to the investigator’s choice group, with the most benefit seen in patients with leiomyosarcoma and liposarcomas. The average length of time to progression for patients with L sarcomas was 5.32 months with aldoxorubicin compared to 2.96 months with other treatments, and the chance of a tumor shrinkage of more than 30% was 10% vs. 4%. Interestingly, there was one patient who did not lose any hair after 20 cycles of aldoxorubicin!
Takeaway – Aldoxorubicin by itself is a reasonable option that is probably better than most other treatments for leiomyosarcomas and liposarcomas. However, we are still only talking about an average of 6 months before the tumors become resistant. But where the benefit really lies is that you can use this drug for much longer with a much lower chance of damaging people’s hearts. Dr. Chawla’s group also reported ongoing results from a smaller study where they combined aldoxorubicin with high doses of ifosfamide. Combining doxorubicin with ifosfamide tends to produce better results than doxorubicin alone. Shrinkages in tumors were seen in nearly 40% of the 18 patients, with stabilization of disease in another 55%. So because of the safety, I think aldoxorubicin makes a lot of sense to include in new combinations for sarcomas where you are using traditional chemotherapy. We’ll have to wait to see what the FDA says.
Read Dr. Chawla’s Aldoxorubicin/Ifosfamide abstract
Next up – Dr. Mrinal Gounder from Memorial Sloan Kettering in NYC presented data from a whopping 5749 patients with 57 different types of sarcoma who had sequencing (mapping of the tumors) performed either through Foundation Medicine or through MSK’s own platform. Take-home points – 8% of sarcoma patients had their diagnosis (specific subtype or sarcoma in general) changed as a result of their sequencing. 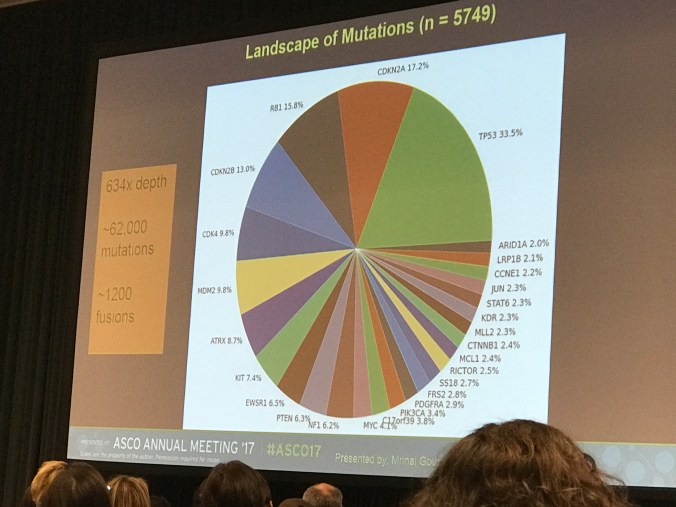 41% of patients had no mutations detected that were matchable to existing targeted drug treatments. 8% had an FDA-approved drug that could be used, 9% matched to an FDA approved drug for a non-sarcoma cancer, and 41% had a mutation that could be matched with up-and-coming investigational drugs. 5% of patients were found to have DNA damage pathways that were affected, which might explain to some degree why the sarcoma happened in the first place. However, he showed several patients where a unique mutation was found that went on to be treated with matched therapies – and they responded.
41% of patients had no mutations detected that were matchable to existing targeted drug treatments. 8% had an FDA-approved drug that could be used, 9% matched to an FDA approved drug for a non-sarcoma cancer, and 41% had a mutation that could be matched with up-and-coming investigational drugs. 5% of patients were found to have DNA damage pathways that were affected, which might explain to some degree why the sarcoma happened in the first place. However, he showed several patients where a unique mutation was found that went on to be treated with matched therapies – and they responded.
Overall, sequencing can be helpful in a fraction of patients to help clarify the diagnosis, and may reveal a potential abnormality that could suggest a new therapy in a very small number of patients. For most patients though, sequencing doesn’t really change the treatment plan much.
In other abstracts, Dr. Steve Attia from Mayo Clinic in Jacksonville, FL reported on SARC024, regorafenib for patients with Ewing sarcomas – incredibly, he reported 3 patients with partial responses (shrinkage of tumors >30%) which lasted for an average of 5.5 months. Over 70% of the 30 patients enrolled did not progress at the two month mark. Crazy for a disease that was thought to be too aggressive for targeted treatments. Dr. Ian Judson from Royal Marsden in the UK presented beautiful data in patient with ASPS treated with cedirinib, showing that nearly 50% of patients who had progressing disease before entry into the study were at least stable at the 12 month mark. And finally, Dr. Javier Broto presented the results of pazopanib for patients with aggressive and malignant solitary fibrous tumors, showing that 40% of the 34 patients enrolled were free from progression at 6 months with therapy. He also showed that these tumors often do not shrink in size, but die internally, so that our typical size-based assessments of activity of drugs often underrepresent benefit – an important lesson for other sarcomas.
Onwards to the immunotherapy abstracts –
Visit my post on Immunotherapy 101 if you need a refresher on the basics!
Dr. Neeta Somaiah from MD Anderson presented the results of a study of CMB305, which is a nifty agent that uses a virus to deliver the protein NY-ESO-1 into the patient’s antigen-presenting cells called dendritic cells. Remember that antigen-presenting cells normally are the cells that recognize foreign proteins, whether it’s the common cold you picked up on the airplane, or cancer cell particles. CMB305 helps to speed up that process by “infecting” the dendritic cells and not relying on them to recognize the cancer cell particles. The virus is combined with a TLR4 agonist that helps to encourage activation and maturation of the infected dendritic cells. This study enrolled 25 patients with sarcomas that express NY-ESO-1. Interestingly, 64% of patients had stable disease, and patient who already had immune cells circulating that had been previously exposed to NY-ESO-1 did much better with the therapy. The treatment could also stop tumor growth, in patients with tumors that were growing at the time of study entry, even though it was not enough to shrink them. CMB305 is now being studied with or without atezolizumab, a PD-L1 checkpoint inhibitor, to see if the activity can be boosted anymore. Very cool. The most common sarcomas that express NY-ESO-1 include synovial sarcoma and myxoid-round cell liposarcomas, with a small percentage of other types of sarcoma which can also express it occasionally. In general this is not a protein that is routinely tested, so it’s important that patients with synovial sarcoma and myxoid-round cell are aware that this treatment, and others that target NY-ESO-1 may be good options for them to consider.
Another NY-ESO-1 directed strategy is the use of NY-ESO-1 engineered T cells. In this method, the patient’s own T cells are harvested, and engineered in a laboratory to be specifically targeted at NY-ESO-1. They are expanded and grown into billions of cells, which are then returned to the patient after chemotherapy which helps to decrease competing T cells and allow the new cells to take root. This method has been studied for patients with NY-ESO-1 positive synovial sarcomas over the past several years. Dr. Sandra D’Angelo from MSKCC presented the updated results for the study, sponsored by Adaptimmune. Up to 50% of patients showed responses in a cohort combined with cyclophosphamide and fludarabine chemotherapy, with one patient with a complete response. Read Dr. D’Angelo’s Abstract.
Next, Sandra D’Angelo showed the first data from the highly anticipated study of the two checkpoint inhibitors, ipilimumab and nivolumab, for advanced sarcomas. Remember, checkpoint inhibitors serve to block the “don’t eat me” signals on cancer cells that shut off the immune system and keep it from attacking. 85 patients were randomized to either nivolumab, or the combination of ipilimumab and nivolumab. One of the worries with the combination is the high rate of immune-related side effects that have been seen in trials with melanoma, non-small cell lung cancer and other cancers. Whereas these older studies showed that 60-70% of patients had severe immune side effects, with Dr. D’Angelo’s study, patient received a lower dose of ipilimumab, and only 14% of patients experienced these more severe toxicities. There were three partial responses (>30% decrease in tumor size) in the nivolumab only arm, in patients with ASPS, leiomyosarcoma, and unspecific sarcoma. In the combination ipilimumab and nivolumab arm, there were 2 patients with complete responses (disappearance of all disease) in uterine leiomyosarcoma and myxofibrosarcoma, and 5 partial responses in leiomyosarcoma, undifferentiated pleomorphic sarcoma, and angiosarcomas. 18% of patients had at least stable disease or better in nivolumab alone, while 29% had stable disease or better in the ipi/nivo group. Again, immune therapies only seem to work for some sarcoma patients, and it’s still not clear how to find these patients. What’s interesting is that leiomyosarcoma was previously thought to not be sensitive to checkpoint inhibitors, but responses were seen in both nivolumab alone as well as the combination. We still have a lot of work to do to figure out how to recognize patients likely to respond, as well as to improve immunotherapy to make it work for more patients.
Finally, Melissa Burgess from the University of Pittsburgh presented the final results from the SARC028 study of the checkpoint inhibitor pembrolizumab for soft tissue and bone sarcomas. The final results were that there were 4 patients with undifferentiated pleomorphic sarcoma who had either a complete response or partial responses, and two patient with partial responses who had dedifferentiated liposarcomas. The study is currently enrolling more patients with these two subtypes for more data. There was one patient with synovial sarcoma who had a partial response but it didn’t last very long, whereas the other patients had long-lasting responses. The most important thing that Dr. Burgess reported was that of the patients who responded, only 2 of them had PD-L1 protein on their tumor cells, 4 of them did not have that marker. This means that unlike other cancers where having PD-L1 on tumors clearly improves the chances for good outcomes with checkpoint inhibitors, this does NOT appear to be the case for sarcomas.
What’s good to know is that we are making slow progress on looking for OTHER signals that can help us identify patients who might respond to immunotherapy. Dr. Seth Pollack from Fred Hutchinson Cancer Center in Seattle recently published an important paper where he identified that PD-L1 expression, clonal populations of T cells, and upregulation of particular immune-related genes all clustered together in sarcoma tissue samples. Read paper here. While he hasn’t shown that this cluster predicts response to immunotherapy, that’s what needs to be looked at next.
The other exciting thing is that pembrolizumab was recently approved for all cancers that have something called microsatellite instability (MSI), where it produced responses in an astounding 53% of patients, with 21% of patients having complete responses. Read the New York Times article. This basically means that the cancer has a fundamental difficulty in repairing mistakes that happen in the DNA that codes them, due to a broken mismatch repair pathway. In another abstract presented at ASCO, Dr. Salah and colleagues from Princess Margaret Hospital in Toronto reviewed immune activity in 18 cases of alveolar soft part sarcoma. Read Dr. Salah’s abstract. 4 patients with ASPS who were treated with PD-1 checkpoint inhibitors had either complete response (1 patient), partial responses (2 patients), or stable disease. Genetic data suggested that the mismatch repair pathway could be affected in 2 of these 4 patients. There are other sarcomas that have also been found to have MSI or mismatch repair deficiencies, and with the recent approval, one could make the argument that we should add this to our list of diagnostics when screening sarcoma patients since this would allow access, and possibly predict good outcomes, to immunotherapy for these patients.
All in all, what an incredible ASCO! Lots of work to do!

Left to right: Robin Jones, me, Min Park, Khin Thway, Jonathan Trent
For more information about ongoing clinical trials for sarcomas, including chemotherapy, targeted therapies, and immunotherapies, check out our ASCO Education Book article. I’ve also uploaded my ASCO slides that covered the current landscape of immunotherapy for sarcomas. ASCO 2017 IT for sarcoma Education Session.

Fascinating and exciting. Great job explaining it all.
LikeLike
I couldn’t make it to ASCO this year. Thank you for a a great summary. Exactly
what I was looking for !
LikeLike
Thanks very much! Fantastic and timely update.
LikeLike